Compensating for Scapular Weakness
“The sole function of the shoulder is to position the wrist and hand. Due to the complex anatomy of the shoulder girdle, our bodies can compensate in incredible ways.”
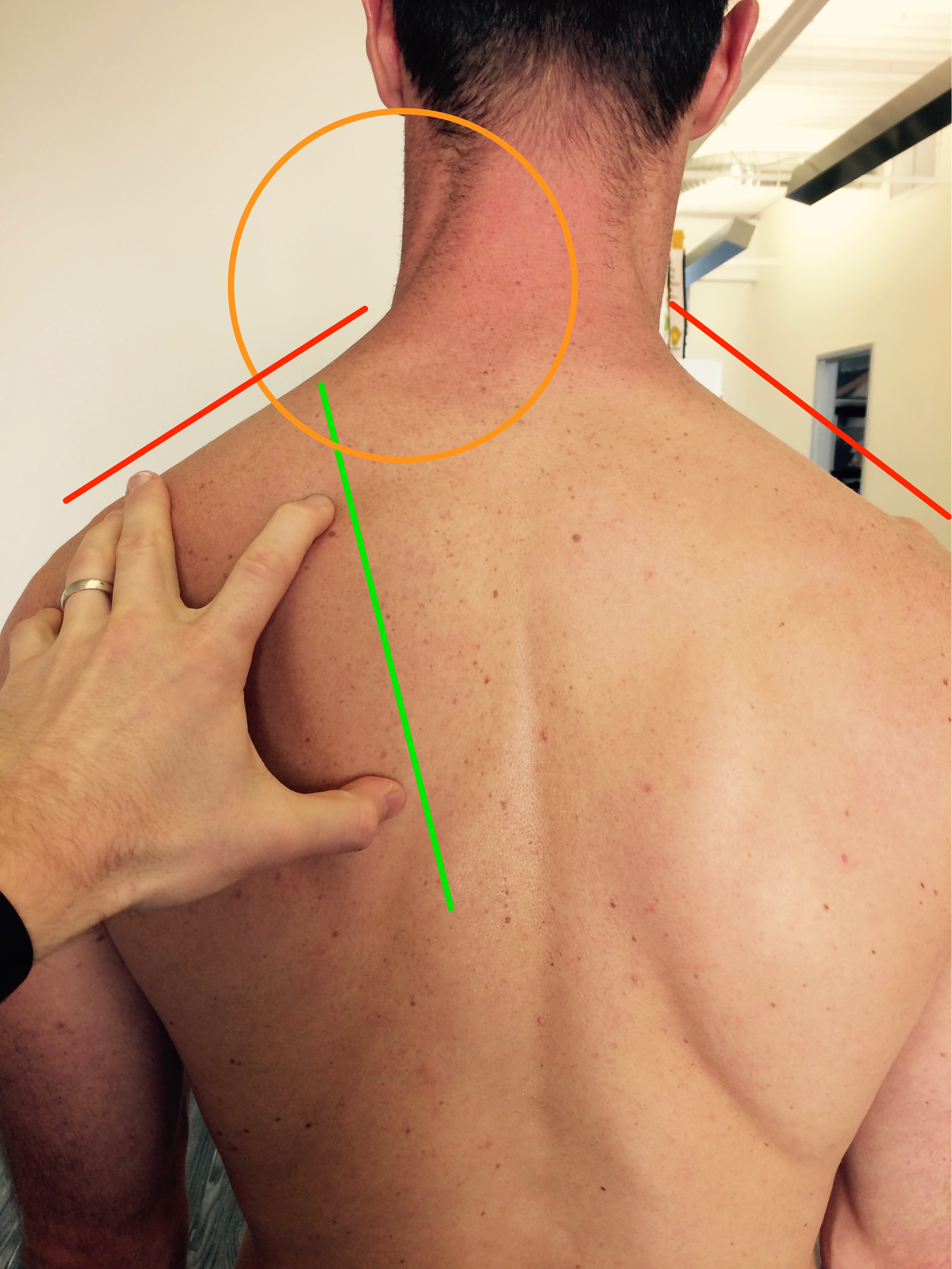
Scapular downward rotation indicated by the inferior border resting closer to the vertebrae than the spine of the scapula.
Overview
The shoulder is arguably the most complex region of the body. It is comprised of the AC, SC, Scapulothoracic, and Glenohumeral joints. Over 15 muscles attach directly onto the scapula, some small stabilizers and other large multi-joint movers.
While there is mixed literature regarding the link between scapular dyskinesias and shoulder dysfunction, understanding scapular mechanics is important when examining someone with shoulder pathology. For example, if someone lacks Serratus Anterior (SA) motor control, it can manifest as the shoulder impingement syndrome (SIS). Good SA strength is essential for normal upward rotation and posterior tipping of the scapula during overhead lifting or reaching. Clinically when a patient lacks SA strength or motor control, the patient may present with shoulder pain, neck pain, thoracic dysfunction and/or rib dysfunction. While movement based diagnosis have their limitations, assessing static and dynamic scapular posture can provide important regarding the patient's symptoms. In the picture above, the scapula is downwardly rotated as evidenced by the inferior angle being more medial than the spine of the scapula. Biomechanically, we can infer that the rhomboids and levator scapulae are placed in shortened position. As the person attempts to raise their arm overhead, the relative tension in the downward rotators limits full upward rotation of the scapula. While this information alone does not determine if someone will have pain, identifying the impairment can lead to an appropriate treatment technique.
“The AC, SC, scapulothoracic, and glenohumeral joints all make up the shoulder complex. Over 15 muscles attach directly onto the scapula.”

How People May Compensate for Scapular Weakness
When the scapular stabilizers are not functioning properly, the body develops creative strategies to complete necessary daily movements. Below I explain two common compensations commonly seen in the Orthopedic population.
Thoracic Extension Compensation
The patient may compensate with excessive lower thoracic extension. With increased lower thoracic extension, the thoracic paraspinals activate to complete the movement. Each time the scapular stabilizers attempt to contract, the thoracic spine locks into extension by using the paraspinals. With this misalignment it will appear that the patient is hinging from the thoracolumbar junction as they perform shoulder movements. To retrain the normal shoulder mechanics, the practitioner need to focus on core position first. Retraining will often need to happen in a gravity eliminated position because the patient will have difficulty isolating the scapular movements.
Scapulohumeral Compensation
The patient will excessively use the scapulohumeral muscles (infraspinatus, teres major, teres minor) without appropriate stabilization from the thoracoscapular muscles. In other words, they will use larger muscle groups to complete a movement without proper stability at the scapula. A common example I see clinically is overuse of the shoulder external rotators with an inability to set the scapula. For example, picture someone performing shoulder external rotation with their arm by their side. As the client performs the movement, the scapula immediately adducts and retracts as the humerus rotates. If the scapular cannot stabilize, the humerus has difficulty remaining centered in the glenoid. To retrain this movement pattern, focus on strengthening the scapular stabilizers (middle trapezius, lower trapezius) in a neutral scapular position first.
While scapular compensations can happen is a variety of ways, be sure to assess the strength and motor control of the scapular stabilizers. Cluster this information with findings from your movement examination. With each painful movement, provide verbal or tactile cues to see if the patient's pain is altered.
Jim Heafner PT, DPT, OCS
Enjoy this post?
Dr. Heafner is now offering The Anatomy of Human Movement + his ebook The Guide to Physical Therapy Examination for only $52.00 (SAVE $30!) for a limited time only!